Macrocytic anemia ICD 10 coding can look simple at first. A provider writes anemia. The lab report shows a high MCV. The patient may have low vitamin B12, low folate, liver disease, alcohol use, thyroid disease, or another health issue. The coder then has to decide if the claim needs D53.9, one of the D51 codes, D64.9, or another code.
This is where many claim errors start. Macrocytic anemia is not a final code by itself in many cases. It is often a lab based description. The red blood cells are larger than normal. That detail helps the provider look for the cause, but the coder still needs clear provider documentation before choosing the final diagnosis code.
For current ICD 10 use, CMS lists official ICD 10 files and the FY 2026 ICD 10 CM guidelines on its ICD 10 page, and the CDC page states that ICD 10 CM guidelines support the rules and instructions found in the Tabular List and Alphabetic Index. For one official coding reference, see the CMS ICD 10 page here: CMS ICD 10 coding resources.
Why Macrocytic Anemia Coding Causes So Many Errors
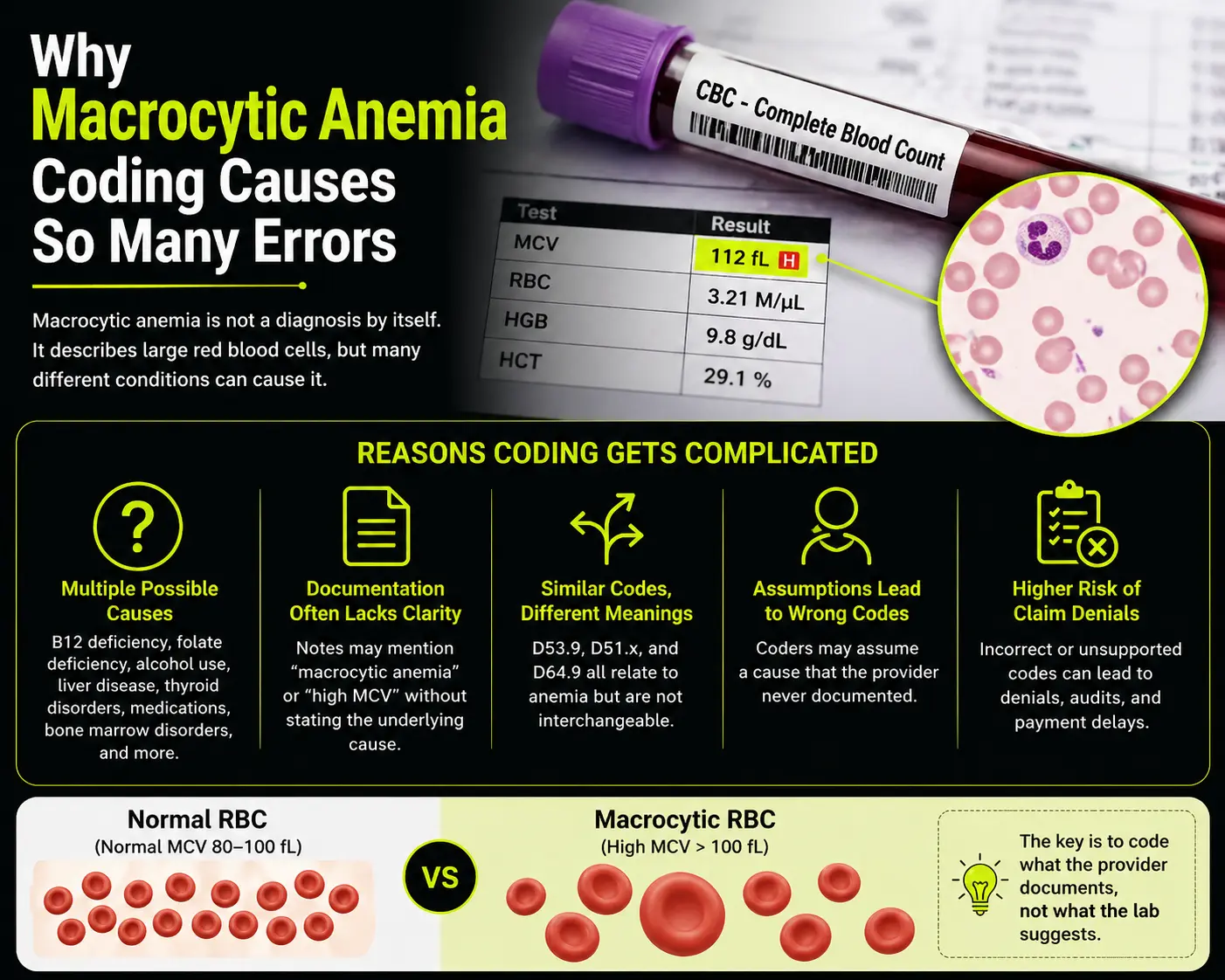
Macrocytic anemia means the patient has anemia with large red blood cells. The term points to the red cell size, not always the exact cause. Many coders see macrocytic anemia and jump to a nutritional anemia code. That can be wrong when the provider has not linked the anemia to a nutrient problem.
A high MCV does not always mean vitamin B12 deficiency. It can happen with folate deficiency, alcohol use, liver disease, some drugs, thyroid disease, bone marrow disease, and other causes. A coder should not pick a cause just because it seems likely. The provider must name the cause or clearly link it in the note.
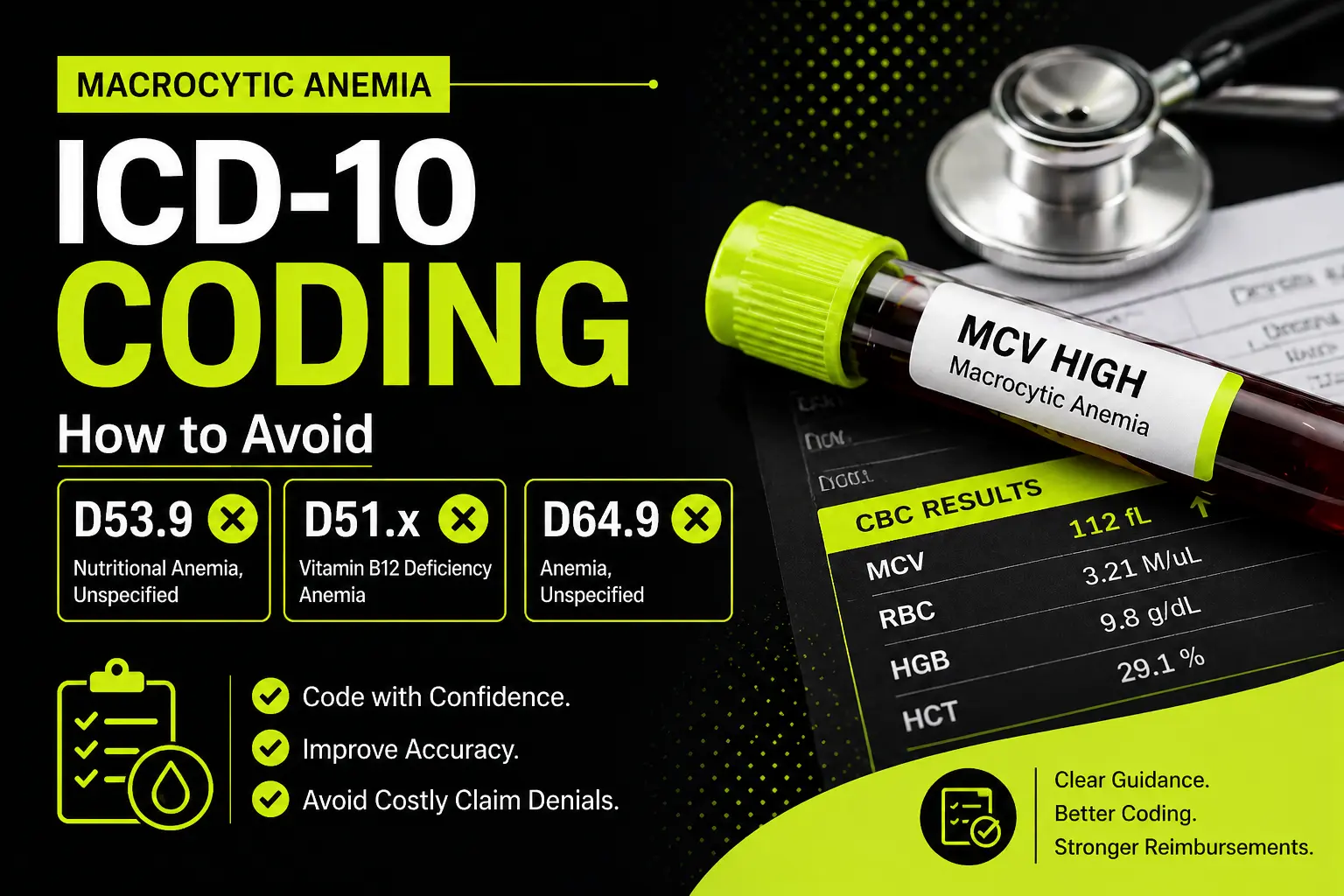
This is why D53.9, D51.x, and D64.9 create confusion. D53.9 means nutritional anemia, unspecified. D51 codes describe vitamin B12 deficiency anemia. D64.9 means anemia, unspecified. These codes do not mean the same thing, and using one as a shortcut can cause weak coding, payer questions, or claim denial.
The Main Rule: Code What the Provider Documents
Good coding starts with the provider note. A lab result can support the note, but it does not replace the provider diagnosis. If the provider documents macrocytic anemia only, the coder should not assume B12 deficiency. If the provider documents vitamin B12 deficiency anemia, the coder can look to the D51 code family. If the provider documents nutritional anemia but does not state the exact nutrient, D53.9 may fit.
This rule protects the claim. It also protects the practice during audits. Payers want the diagnosis code to match the medical record. When the chart does not support the code, the claim becomes easy to question.
The safest habit is simple. Read the assessment and plan. Check the lab comments. Look for the provider’s link between anemia and the cause. If the link is missing, ask for clarification when your policy allows it.
What D53.9 Means and When It Goes Wrong
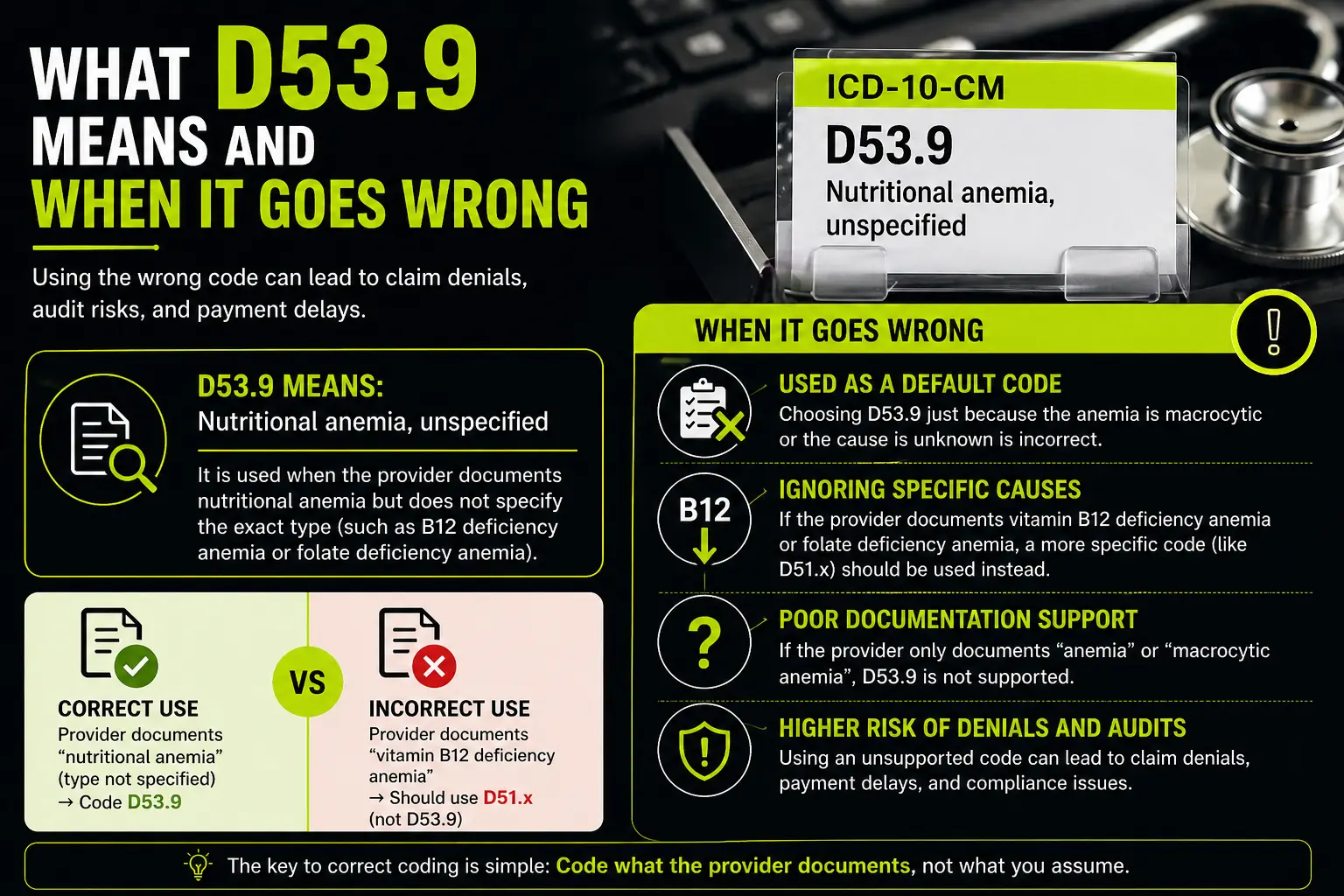
D53.9 stands for nutritional anemia, unspecified. It is not a general code for all macrocytic anemia. It should point to anemia caused by a nutrition related issue, but the provider has not named the exact type.
This is the first common D53.9 coding mistake. A coder sees large red cells and thinks nutrition. The provider may have ordered B12 and folate tests, but that does not mean the provider diagnosed nutritional anemia. Ordering a test is not the same as naming the condition.
D53.9 may fit when the note says nutritional anemia and gives no further detail. It may also fit when the provider says macrocytic anemia likely due to nutritional deficiency but has not named B12 or folate. Even then, the coder should follow local policy and payer rules because words like likely may need careful review.
D53.9 should not act as a backup code when the chart only says anemia. It should not replace D64.9 when the provider gives no cause. It should not replace D51 codes when the provider clearly states vitamin B12 deficiency anemia.
The goal is not to avoid D53.9 every time. The goal is to use it only when the record supports it.
What D51.x Means and Why It Needs Clear B12 Documentation
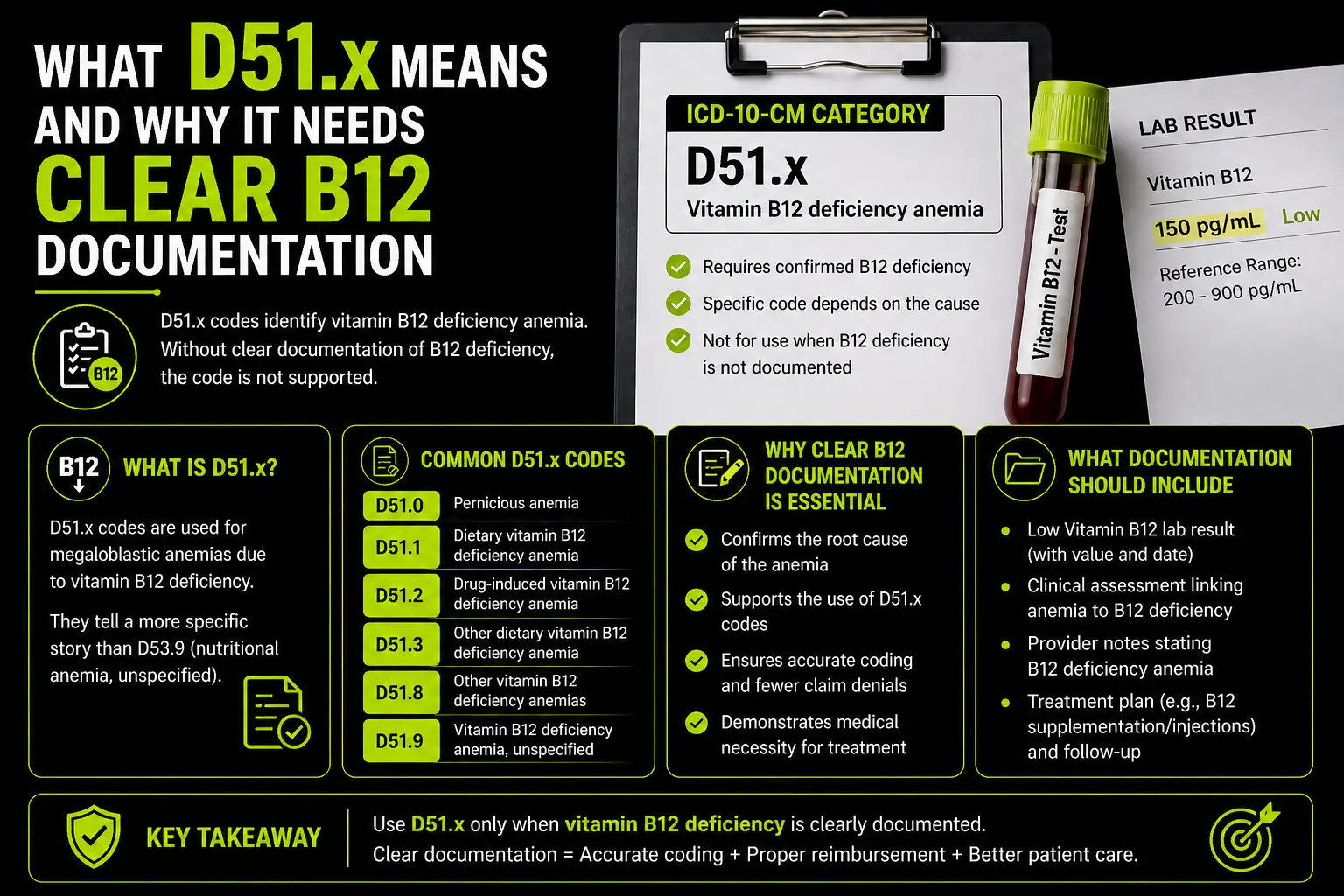
The D51 code group describes vitamin B12 deficiency anemia. This is more specific than D53.9. If the provider states vitamin B12 deficiency anemia, the coder should not stop at D53.9. The record gives a clearer cause, so the claim should reflect that cause.
The phrase D51.x ICD 10 often appears in coding searches because there are several D51 choices. Some describe pernicious anemia. Some describe dietary B12 deficiency anemia. Some describe other B12 deficiency anemia. Some describe vitamin B12 deficiency anemia without more detail.
This matters because not every B12 problem is the same. A patient may have poor intake. Another patient may have malabsorption. Another may have pernicious anemia. The provider note should guide the final code.
A low B12 lab by itself does not always mean the coder can assign a D51 code. The provider must diagnose the condition. The note should say vitamin B12 deficiency anemia, pernicious anemia, dietary B12 deficiency anemia, or another clear B12 related anemia diagnosis.
If the provider only says macrocytic anemia and low B12, many offices will ask for clarification before assigning a D51 code. This keeps the claim cleaner and reduces risk.
What D64.9 Means and Why It Is Often Overused
D64.9 means anemia, unspecified. This code has a place. Use it when the provider documents anemia and does not give the type or cause. It may feel too broad, but it can be the correct code when the record gives no more detail.
The problem starts when D64.9 anemia unspecified becomes a habit. Some billers use it for every anemia case because it is easy. That can cause poor data, weak medical need, and more payer review. Many services need a more exact diagnosis to show why the test, drug, visit, or treatment was needed.
D64.9 should not be used when the provider clearly states vitamin B12 deficiency anemia. It should not be used when the provider clearly states folate deficiency anemia. It should not be used when the note links anemia to chronic kidney disease, cancer treatment, blood loss, or another named cause.
D64.9 is not wrong just because it is unspecified. It is wrong when the chart supports a better code and the coder ignores it.
Macrocytic Anemia Does Not Always Mean D53.9
This is one of the biggest points in macrocytic anemia coding. Macrocytic describes red cell size. Nutritional anemia describes a cause. These are not the same thing.
A patient can have macrocytic anemia from B12 deficiency. Another patient can have macrocytic anemia from folate deficiency. Another patient can have macrocytic anemia linked to alcohol use or liver disease. Another patient can have macrocytosis without clear anemia. The code must follow the provider’s final diagnosis.
If the provider says macrocytic anemia due to folate deficiency, the coder should review the folate anemia code options. If the provider says macrocytic anemia due to vitamin B12 deficiency, review D51 codes. If the provider says macrocytic anemia, cause unknown, the coder may need an unspecified anemia code or a query, based on office policy.
Never let the lab value do the provider’s job. MCV can guide the provider, but the diagnosis in the note guides the coder.
Common Documentation Clues That Help Coding
The best notes give the coder a direct link. A strong note may say vitamin B12 deficiency anemia. It may say macrocytic anemia due to folate deficiency. It may say pernicious anemia. It may say anemia related to chronic alcohol use. It may say anemia due to chronic kidney disease.
A weak note says anemia only. A weak note may also say high MCV with no final diagnosis. A weak note may list B12 test ordered, folate test ordered, and follow up planned, but it does not state the cause.
When the note is weak, do not guess. Check whether the provider gave a final diagnosis elsewhere in the encounter. Look at the problem list only if your coding policy allows it for that setting and payer. Review past notes when they are part of the record and support the current visit. If the cause still remains unclear, send a clear query.
A Simple Way to Choose Between D53.9, D51.x, and D64.9
Start with the exact words in the provider note. If the note says anemia only, D64.9 may fit. If the note says nutritional anemia but does not name B12, folate, or another type, D53.9 may fit. If the note says vitamin B12 deficiency anemia, review D51 codes.
If the note says macrocytic anemia only, do not jump straight to D53.9. Ask what the provider has actually diagnosed. Macrocytic anemia is not the same as nutritional anemia. If the provider did not name the cause, the coder should not name it for them.
If the note says low B12 but does not say B12 deficiency anemia, the coder should be careful. A lab finding and a diagnosis are not always the same. Ask for a provider link if needed.
If the note says history of B12 deficiency but the current visit only treats anemia with no clear link, review the full record. A history code or current condition code may depend on whether the condition still exists and affects care.
Struggling with Macrocytic Anemia ICD 10 Coding?
Avoid costly errors and improve claim accuracy with simple, practical billing guidance.
How Claim Denials Happen With These Codes
Denials often happen when the diagnosis does not support the service. For example, a payer may question B12 injections if the chart does not support a B12 related condition. A lab claim may fail when the diagnosis does not meet medical need rules. A visit level may look weak when the diagnosis code is too vague for the care given.
Another denial risk comes from mismatch. The provider note may say anemia, unspecified, but the claim says vitamin B12 deficiency anemia. The payer may ask for records. The record then fails to support the claim. That can lead to takebacks or added work for the billing team.
A third risk comes from overuse of unspecified codes. Sometimes unspecified codes are correct, but repeated use can hide the real reason for care. Better documentation helps coders choose better codes. Better coding helps billers send stronger claims.
How Providers Can Help Billers Code Macrocytic Anemia
Providers can make coding much easier by using clear words. Instead of writing macrocytic anemia only, they can write macrocytic anemia due to vitamin B12 deficiency when that is the final diagnosis. They can write folate deficiency anemia when folate is the cause. They can write anemia, cause not yet known when the workup is still in progress.
The note should also show the plan. If the provider orders B12 testing, folate testing, thyroid testing, liver tests, or a blood smear, the plan tells the story. But the final code still needs the diagnosis.
When providers link the cause, coders do not have to guess. This saves time, reduces queries, and improves claim quality.
How Billers Can Reduce Coding Mistakes
Billers and coders can reduce mistakes by building a simple review habit. First, read the diagnosis line. Then read the assessment and plan. Then check the lab support. Then match the most specific supported code.
Do not code from the lab page alone. Do not code from the order alone. Do not code from memory. Always let the record drive the code.
It also helps to keep a small internal guide for anemia codes. The guide can remind staff that D51 codes need B12 deficiency anemia, D53.9 needs unspecified nutritional anemia, and D64.9 needs unspecified anemia. Keep the guide simple so the team uses it.
Better Words to Look for in the Medical Record
Clear words include vitamin B12 deficiency anemia, pernicious anemia, dietary B12 deficiency anemia, folate deficiency anemia, nutritional anemia, anemia of chronic disease, anemia in chronic kidney disease, acute blood loss anemia, and anemia due to chemotherapy.
Unclear words include anemia, macrocytosis, high MCV, abnormal CBC, low hemoglobin, low B12, and low folate. These words may support more review, but they do not always give enough detail for a specific anemia code.
This is where human review matters. Coding tools can suggest codes, but they can also suggest codes too fast. A trained coder sees the difference between a lab clue and a provider diagnosis.
Example One: Macrocytic Anemia With Low B12
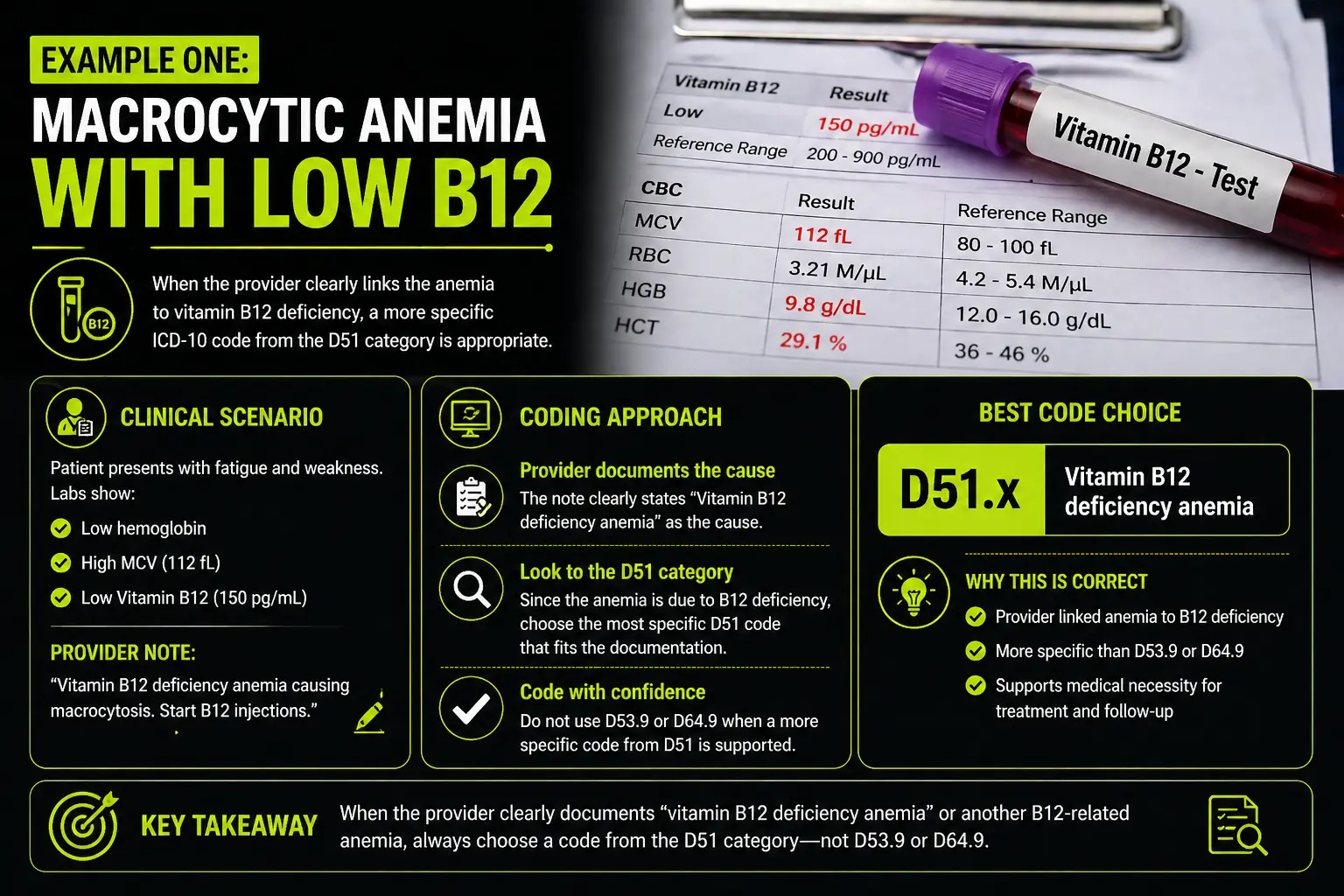
A patient comes in with fatigue. Labs show low hemoglobin, high MCV, and low vitamin B12. The provider writes macrocytic anemia, start B12 shots.
This note may still need more clarity. The provider did not clearly write vitamin B12 deficiency anemia. Many coders would ask the provider to confirm whether the anemia is due to B12 deficiency. If the provider confirms it, a D51 code may fit.
Now change the note. The provider writes vitamin B12 deficiency anemia causing macrocytosis, start B12 shots. This is much stronger. The coder can now review the D51 code choices and select the best match.
Example Two: Macrocytic Anemia With No Cause Yet
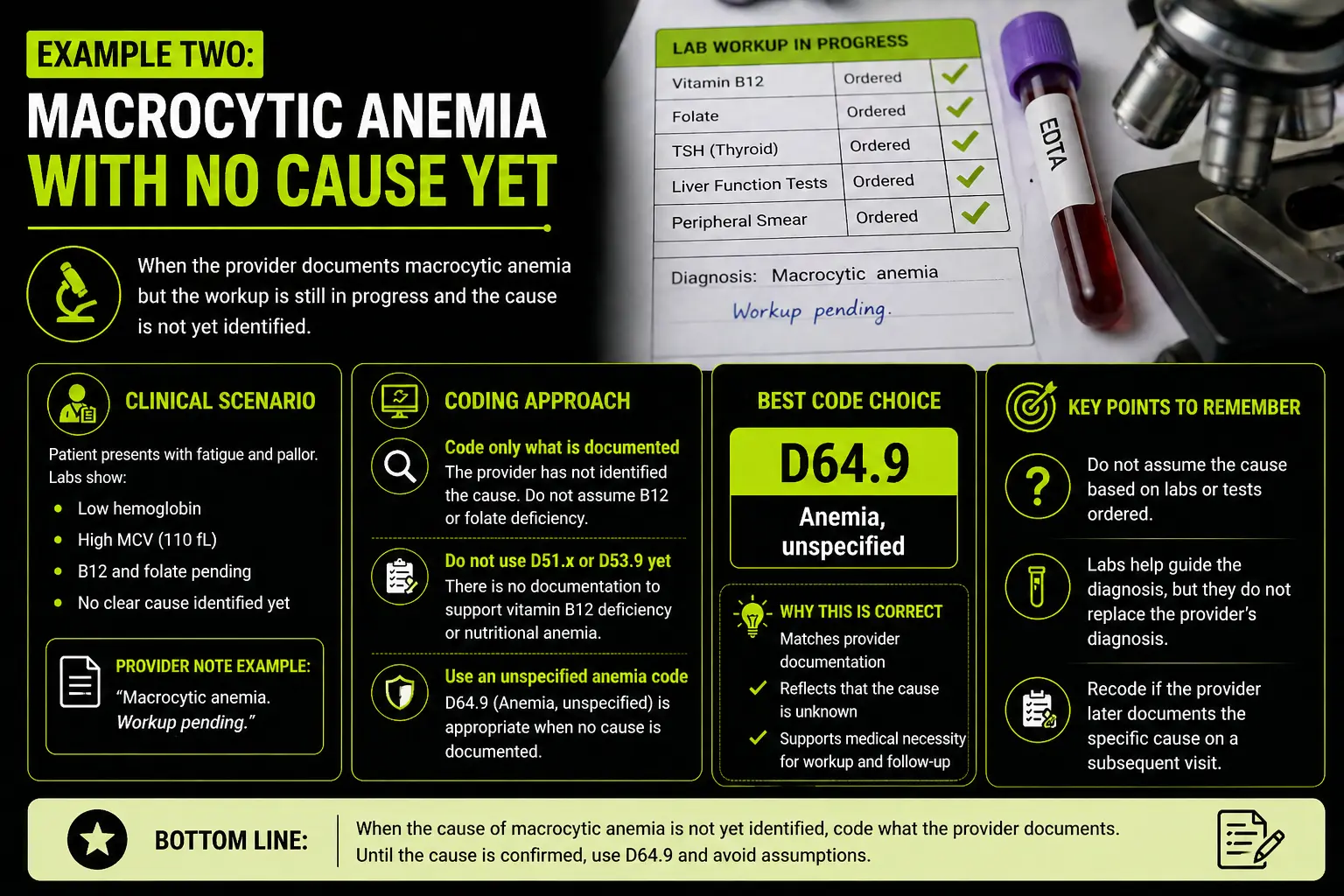
A patient has anemia and high MCV. The provider orders B12, folate, thyroid, and liver tests. The note says macrocytic anemia, workup pending.
In this case, the provider has not named the cause. The coder should not assign D51 just because B12 testing was ordered. The coder should not assign D53.9 just because nutritional causes are being checked. The provider has not said nutritional anemia.
Depending on the record and payer rules, an unspecified anemia code may be the best supported choice until the provider names the cause. The coder can also query if the claim needs more detail and the policy allows it.
Example Three: Nutritional Anemia Without Details
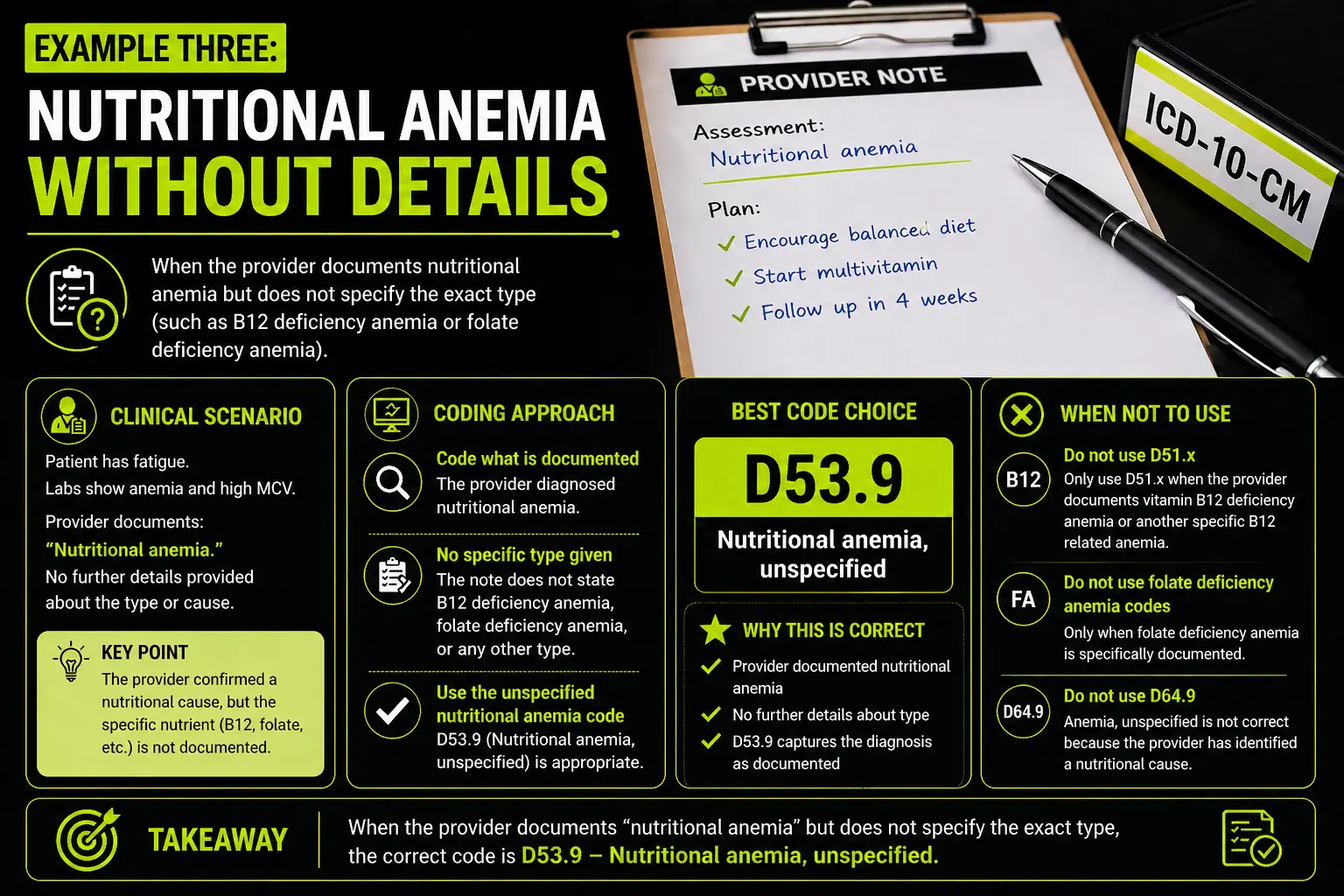
A provider documents nutritional anemia and tells the patient to improve diet. The note does not say B12 deficiency. It does not say folate deficiency. It does not name another exact nutrient.
This is where D53.9 may fit because the provider gave a nutritional cause but did not give the exact type. The code is not a default. It works only because the provider used words that support nutritional anemia.
Example Four: Anemia Only
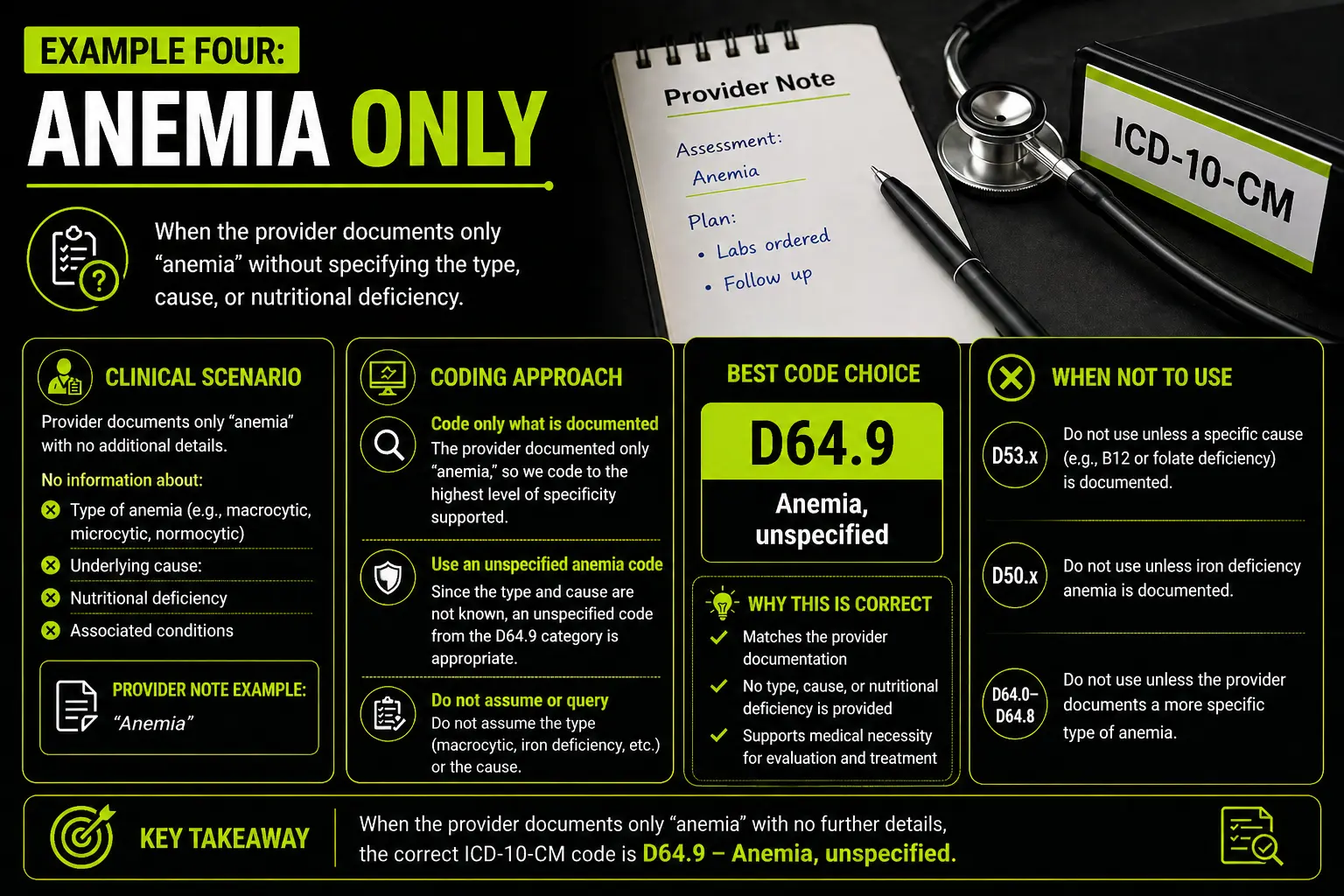
A provider writes anemia and orders a complete blood count follow up. The note does not state macrocytic anemia, B12 deficiency anemia, folate deficiency anemia, or nutritional anemia.
This is a common case for D64.9 if no other detail appears in the record. The code may be vague, but it matches the note. The right long term fix is better documentation, not guessing.
Why Specific Coding Helps the Whole Revenue Cycle
Specific coding helps more than the coder. It helps front office staff, billing staff, payment posters, denial teams, and compliance teams. A clean diagnosis helps show why the provider ordered tests, gave treatment, or asked for follow up.
For medicalbilling.help readers, this is a key point. Better coding does not start after denial. It starts in the chart. When the diagnosis code matches the provider note, the claim has a stronger chance of moving through the payer system with less trouble.
Specific codes also help patient records. They show the true reason for care. This matters when the patient returns, changes providers, or needs long term care.
How to Write a Good Query for Macrocytic Anemia
A good query stays clear and does not lead the provider. It should ask for the cause only when the record supports the need for clarity. It should show the facts from the chart, such as anemia, high MCV, low B12, or treatment plan. It should let the provider choose the right diagnosis.
The query can ask whether the macrocytic anemia is due to vitamin B12 deficiency, folate deficiency, another cause, or an unknown cause. The provider should answer in their own words.
A query should never push the provider to choose a higher paying code. The goal is truth, not payment only. Clean coding follows clear care.
Final Coding Tips for D53.9, D51.x, and D64.9
Use D51 codes when the provider documents vitamin B12 deficiency anemia or another clear B12 related anemia diagnosis. Use D53.9 when the provider documents nutritional anemia but does not name the exact type. Use D64.9 when the provider documents anemia without a type or cause.
Do not use D53.9 only because red cells are large. Do not use D51 codes only because B12 is low. Do not use D64.9 when the note supports a more specific anemia diagnosis.
Macrocytic anemia ICD 10 coding becomes easier when you slow down and ask one question. What did the provider diagnose today? The answer to that question should guide the claim.
FAQ
What is the best ICD 10 code for macrocytic anemia?
There is no single best code for every macrocytic anemia case. The best code depends on the cause documented by the provider. If the provider states vitamin B12 deficiency anemia, review D51 codes. If the provider states nutritional anemia without more detail, D53.9 may fit. If the provider only states anemia, D64.9 may fit.
Can I use D53.9 for all macrocytic anemia cases?
No. D53.9 means nutritional anemia, unspecified. Macrocytic anemia can have many causes. Use D53.9 only when the provider documents nutritional anemia or clearly supports an unspecified nutritional cause.
When should I use D51.x codes?
Use D51 codes when the provider documents vitamin B12 deficiency anemia or a specific B12 related anemia such as pernicious anemia. A low B12 lab alone may not be enough unless the provider also diagnoses the condition.
Is D64.9 always a bad code?
No. D64.9 is correct when the provider documents anemia and gives no type or cause. It becomes a problem when the record supports a more specific code and the coder still uses D64.9.
Can lab results decide the anemia code?
Lab results can support the provider note, but they should not replace the provider diagnosis. The coder should not choose a cause from lab values alone.
What should I do if the note says macrocytic anemia with workup pending?
Do not guess the cause. Code only what the provider has documented. If your office policy allows it and the claim needs more detail, send a query for clarification.
Why do payers deny claims with anemia codes?
Payers may deny claims when the diagnosis does not support the service, when the code is too vague for the treatment, or when the record does not match the code on the claim. Clear documentation and specific coding can reduce this risk.